When Most Tests Can’t be Done
A Psychologist Questioned:
So yesterday I had a 50 y o Down’s Syndrome woman with her mother in for eval of possible AD.
The young lady refused to cooperate and after an hour of interview and observation, we gave up. I did try to administer the MMSE which I thought would be relatively easy for her, but to no avail,
Can I bill for this?
Do I just chalk it up to one hour of interview?
Do I enter her “data” into the panorama program?
Or do we just walk away with a letter to the mother, MD, and her residential program?
Answers:
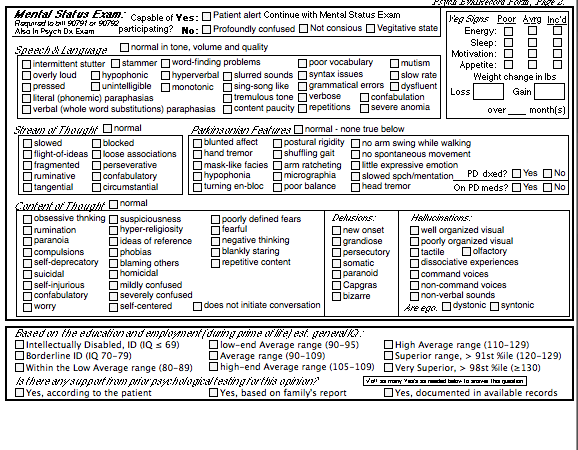
All your suggestions are appropriate, but here’s a solution using the available codes for which you met criteria. Usually, we include interviewing and record review within the first hour of testing. However, in this case since the emphasis was on diagnostic interviewing rather than test administration, to maximize the billing you could use the Nonmedical Psychiatric Diagnostic IV code 90791 which we testers rarely use, but it is used for all intakes of therapy cases. 90791 is untimed and aimed at history and a mental status exam; BTW– this is not the MMSE as this 90791 is based on, Medical Psy. Dx IV 90792, which was designed for psychiatrists whose evaluation is primarily interview based. Now you understand why Protocol #2 has this section (shown below) which we testers rarely use, but it is there to support code 90791/2. You should complete the Mental Status Exam (shown below) on your patient if you bill 90791 which pays better* and takes no time away from your testing billing.
I can’t remember, but at times there has been an issue with using 90791 on the same day as testing which I don’t think applies now. You can’t bill 90791 on the same day to you psychotherapy codes with a patient, however.

Eventually you probably gave up and quit attempting tests. For those unattempted tests, check off “Not Done” so the scoring program will run. Those tests will not show up in the Tests Administered section of the report.
In the report, after you score it, mark “Skip Page” to disregard the pages that are mostly blank due to no testing done. You’ll need at least page one for history and tests given, page two of observations, the page the MMSE shows up on and likely the last page with your diagnostic impression (mostly based on interview and report I’d guess) and recommendations.
Billing:
Billing for test services is broken up into three sections, each of which consists of a “base” code followed by “add-on” services if needed. Think of it like:
Pre-testing Planning/Setup: 96132–one hour
Testing Administration/Scoring 96136–first 1/2 hr + 96137–each add-on 1/2 hr
Post-testing Interpreting/Report Writing: 96133–each hour
It is unbelievably complex. There used to be one code for neuropsychological testing, but in their wisdom the APA fought to get Medicare to pay more for planning and interpretation as opposed to test administration. So this resulted in a few more dollars for 96132 and 96133 as compared to 96136, and as the first half hour of testing is more work than adding on additional half hours of 96137 yields a few cents less than. So to make a little more we spend hours in complex billing manipulation and audit defense which turned out to be a nightmare. So we use a computer, and it took hundreds of hours to figure this out and write that program.
OK, now you should bill 96132 which is basically for planning in advance, setting up, “thinking” about the case and your initial contacts and initial testing. This typically includes your interviewing. 96132 is for the first hour or 60 minutes and some of that occurred before the patient arrived as you prepared. To bill it you need to have spent at least 31 minutes on this service. (Since it overlaps with seeing the patient we required you spend 60 minutes to bill this; however, it is a reasonable hypothesis that if you did 96132 on a prior day to seeing the patient in person then ≥31 minutes would allow its billing. Note there is a separate date for 96132 that could be used for this purpose. Still we take a conservative approach and ask you to spend a full 60 minutes on this code.)
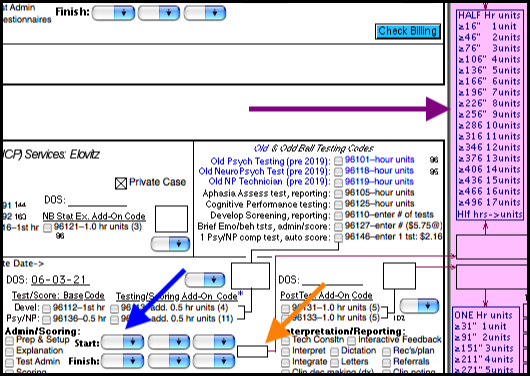
Next, bill for any testing/scoring. For the first 0.5 hr of face-to-face contact and scoring with the patient, 1 unit of 96136. Lets say you spent more than a half hour testing/scoring. If you spent an additional ≥16 minutes but less than 46” bill 1 unit of 96137; if you spent ≥47” but ≤75” bill 2 units of 96137 and so on. This is why there is this chart (purple arrow, below) to help you figure this nightmare stuff, but of course the computer will calculate it for you (orange arrow) if you just enter in your Start and Finish times (blue arrows).
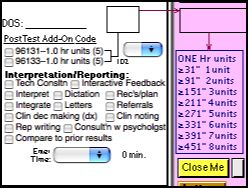
Finally, you had to interpret and write up the results. If this took at least 31 minutes you’d bill 1 unit of 96133, if you spent ≥91”
Jerry
*If you want to hassle a bit, remember in your list of billing to Art to note you did a 90791 as (I think) it pays $70. Art could likely break it out and you get a bit more money tom compensate for losing on the overall testing since she wouldn’t cooperate.
